
| Joint capsule | |
|---|---|
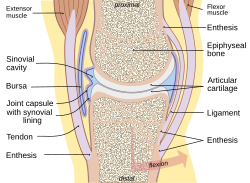 Typical joint | |
 Diagrammatic section of a diarthrodial joint. | |
| Details | |
| Identifiers | |
| Latin | capsula articularis |
| MeSH | D017746 |
| TA98 | A03.0.00.026 |
| TA2 | 1536 |
| FMA | 34836 |
| Anatomical terminology | |
In anatomy, a joint capsule or articular capsule is an envelope surrounding a synovial joint.[1] Each joint capsule has two parts: an outer fibrous layer or membrane, and an inner synovial layer or membrane.
YouTube Encyclopedic
-
1/3Views:216 42678026 537
-
Shoulder Joint - Human Anatomy | Kenhub
-
Shoulder Joint Anatomy and Function - Glenohumeral Joint - Capsule - Bursae - Movement
-
Hip joint - blood supply, innervation and bones - Human Anatomy | Kenhub
Transcription
Hello everyone! This is Joao from Kenhub. Today, I'm doing a tutorial on the shoulder joint, as you can see already from the images that are displayed on your screen. And what I'm going to do is talk about the most mobile joint in your body but also the one that is most susceptible to injury. You have probably heard of someone close to you that has had some sort of shoulder dislocation. Now, what you have on the screen, on your left, you will find the posterior side of the joint, and on your right, you can find the anterior view of the shoulder joint. One thing that you need to know about this joint is about the type. This is a synovial joint, a ball-and-socket, which, as you know, ball-and-socket joints have great freedom of movement. Now, let's start talking also about the articulating surfaces. The articulating surfaces of the shoulder joint is the head of the humerus, the rounded head of the humerus, and also the shallow and pear-shaped glenoid cavity of the scapula. Keep in mind that both these articulating surfaces are covered by hyaline cartilage—very important. Another characteristic about these two articulating surfaces is that the head of the humerus is about three to four times larger than the articular surface of the scapula or the glenoid cavity. That is why, to help correct this difference, you're going to find on the edges of the glenoid cavity a fibrocartilage rim as I'm drawing right now. This fibrocartilage rim is known as the glenoidal lip or the glenoid labrum. Now, it's important to know that the size of the articulating surfaces have an advantage. It allows an increased range of shoulder motion, but it also has a disadvantage and that is that it compromises the stability of the joint. That's why there is always a lot of problems associated to it. So weak ligaments and capsule, the joint is primarily stabilized by the rotator cuff muscles—another muscles that we're going to see later on this tutorial. As you can see here on this image, I zoomed in on the anterior view of the shoulder joints where I'm going to start talking about a very important feature known as the capsule. And the capsule of the shoulder joint is surrounding the entire joint. And medially, as I'm highlighting here in blue, medially is attached to the glenoid cavity right outside that fibrocartilaginous extension that I talked about on the previous slide known as the glenoid labrum. Now, this will extend. This capsule will extend all the way laterally where it's then going to attach to the anatomical neck of the humerus, and then—as you can see here on this image—will extend just a little bit further down medially to the side of the shaft of the humerus for just a short distance as you can see. Important feature of the capsule is that it's thin and broad, which then allows the wide range of movements that are associated to this joint. Also, it is partially strengthened by ligaments and also by the tendons of the rotator cuff muscles, which we are going to discuss later on on this tutorial in a little bit more detailed. Now, one important feature that I would like to add on the capsule is that if you notice there is a little recess or a little bump that I'm going to highlight here in green. This is when the arm is hanging down. You see that the lower part of the joint capsule which is not reinforced by muscle is sagging and is forming this green structure that I highlighted—was not in green, but is highlighted in green—and it's known as the axillary recess. This provides a reserved capacity that is useful during abduction movements of the arm. As you probably notice, we're still talking about the capsule of the shoulder joint, and from previous knowledge, you know that capsules on synovial joints have two main layers: the synovial layer and the fibrous layer. Both these layers have different or they're comprised of different types of tissues, as well as their location in the capsule is... they are different. So the synovial layer is located in the innermost part of the capsule, usually in contact with synovial fluid, hence the name synovial layer. Now, the fibrous layer is usually located more externally and also has a different composition or comprised of different tissues. Now, knowing that, let's talk about the synovial layer of the capsule of the shoulder joint. This layer is actually attached to that extension that we talked about, this fibrocartilaginous extension known as the glenoid labrum. This is the attachment of the synovial layer. And also, I'm going to add here the muscle of the biceps brachii muscle. As you can see, the long head or the tendon of the long head goes through the intertubercular sulcus on the humerus and then attaches to the supraglenoid tubercle on the scapula. And you can see that the way I highlight it that the capsule or the synovial layer of the capsule surrounds the tendon of the long head of the biceps and extends beyond the transverse humeral ligament. And we're going to talk about this ligament later on, but I can show you and draw that is connecting the two tuberosities. This is where you should find the transverse humeral ligament. Now, this extension of the synovial layer surrounding this tendon, then, is surrounding it as what we call the synovial sheet of the intertubercular groove or sulcus. Now, an important thing to know about the synovial layer as well is that it protrudes usually through the fibrous layer to form the bursae which are important structures, that we will talk about later, that reduce friction on a joint. Now, just a quick note on the fibrous layer, all you need to know is that it forms a connective tissue layer across the intertubercular sulcus and converts it into an osteofibrous canal. So it's time to talk about the ligaments that strengthen and stabilize the shoulder joint. There are six that we're going to talk about on this tutorial. The first one is the glenohumeral ligament as you can see here. This is also divided into three other ligaments or three other weak bands of fibrous tissue: the superior, the middle, and also the inferior glenohumeral ligaments. As you can see here, this is the anterior view of the joint, and for that reason, you know that this ligament is strengthening the front of the capsule, and it's extending from the margin of the glenoid cavity all the way to the lesser tuberosity. Now, I'm going to raise this, so I can show you the fourth ligament. And this is the transverse humeral ligament which is bridging—we talked about on the previous slide—this is bridging the gap between the tuberosities, and it's found more laterally. The other ligament that we need to talk about is the coracohumeral ligament, which stretches from the root of the coracoid process to the greater tuberosity of the humerus as you can see here. And this is strengthening the capsule above or superiorly. The last ligament that we need to talk about, I'm going to try to find it here. It's the coracoacromial ligament, as you can see here, which is connecting the acromium and the coracoid process of the scapula. This is an accessory ligament and is protecting the superior aspect of the joint. And it does so by forming an arch; as you can see here, this is forming an arch, also known as a fornix, above the joint which is preventing superior relaxation of the joint and it restricts the movements of the joint. An example of that is abduction can only happen up to 90 degrees because the greater tuberosity of the humerus, as you can see here on this image right here, will then come into contact with this ligament and prevent from further movement. Now, it's time for us to talk about the muscles that help stabilize the shoulder joint. There are few that we need to discuss because this joint has a few weak ligaments, so we cannot depend on them in order to be stablilized, so it is a muscle-dependent joint. So it depends... its stability depends on the muscles that are surrounding it and are stabilizing it. The very first group of muscles that we need to discuss—they are the most relevant or they play the major role of stabilizing this joint—are known as the rotator cuff muscles. The rotator cuff muscles, there are four. The first one that you can see anteriorly is the subscapularis that origins... or originates (sorry) on the scapula and goes all the way to the lesser tuberosity of the humerus. So that's why you can see that is related to the joint, the shoulder joint. The other three, you can find them on the posterior view, and these are the infraspinatus, as you can see here, and the supraspinatus, and I'm going to clear this two so you can see the other one, which is the teres minor. Both the infraspinatus and supraspinatus origin on the scapula, then, will exert on the greater tuberosity of the humerus. And also the teres minor is originating on the scapula and goes all the way to insert as well on the greater tuberosity of the humerus. Now, I want to show all of these muscles together, so you can see the entire group of the rotator cuff muscles. So we still have here the muscles of the rotator cuff, so I can show you the next muscle that plays a role in stabilizing the shoulder joint, and this is the teres major muscle that I just showed you posteriorly but I will also show you anteriorly, and this is it. And the teres major is inserting on the crest of the lesser tuberosity, and that's why it's also playing a role in stabilizing the shoulder joint. Next muscle that helps stabilize the joint is the coracobrachialis muscle, as you can see here, that originates on the coracoid process of the scapula and goes to insert in the humerus in line with the crest of the lesser tuberosity. That's why it's helping stabilize this joint. The next muscle that helps stabilize the shoulder joint is a very powerful one known as the deltoid muscle as you can see here on the posterior view. And it's better to show it on this side so you can see it in its majority. And you can see that this muscle is originating from the scapula and the clavicle. And I also have another image here that illustrates a little bit better where it's going to insert. And it will insert in the very well-known deltoid tuberosity on the humerus, and that's why this muscle plays a major role not only in stabilizing the shoulder joint but also in a lot of the movements related to this joint. The biceps brachii muscle, as I'm showing here on the image, also influences in stabilizing the joint. As you can see here, the long head or the tendon of the long head passes though the intertubercular sulcus on the humerus and goes and originates, if you notice here, on the supraglenoid tubercle on the scapula. So for that matter, all the movements related to this muscle will then influence or be associated to the movements of the shoulder joint. And of course, this muscle also plays a role in stabilizing it. Now, I'm going to talk about the last two muscles that influence in stabilizing the shoulder joint. And the one that you're seeing here right now is a portion of the latissimus dorsi, and you can see, that is inserting on the crest of the lesser tuberosity of the humerus as you can see here. Now, the other one is a very powerful muscle known as the pectoralis major, and you can see that the pectoralis major is inserting here on the crest of the greater tuberosity of the humerus. The next topic on this shoulder joint tutorial, it's going to be is going to be the bursae. Bursae is plural and bursa is singular. And a bursa is a synovial sac that is filled with fluid that help cushion and also alleviate some friction that is usually associated to synovial joints—very, very important structures. Now, remember from previous topic when we talked about the synovial layer and also the fibrous layer of the capsule, well, the synovial layer usually protrudes through the fibrous layer, and that way, it will form some bursa. Now, on this tutorial, I'm going to talk about four more bursae. And the first one, you can see on this image, we're looking at it anteriorly. And I left some of the ligaments, so you can see where you can find this bursa in relation to these structures. Now, the first one is known as the subcromial and subdeltoid bursa, this green structure that you find here. And you can see it here also posteriorly and a little bit more superiorly. You find also this subacromial—this green structure here—this is the subacromial and subdeltoid bursa. Now there are three other bursae that I need to cover here in this tutorial. What I'm going to do now is highlight the capsule and also the bursa associated with the capsule and to the joint, so you can see where they're located. Now, the first one is this red, highlighted in red, and this is the subcoracoid bursa. The next one is this one highlighted in blue, and this is the subtendinous bursa of the subscapularis muscle. So this is just beneath the tendon of the subscapularis muscle. And the next one, this yellow structure here is known as the intertubercular synovial sac. So this is surrounding the tendon of the long head of the biceps, and you can see it a little bit better on this image here, so I'm going to also highlight it in yellow so you can see that this structure, this intertubercular synovial sac or sheet, is surrounding the tendon of the long head of the biceps and is extending beyond the transverse humeral ligament that you can see better on this image. Here is the transverse humeral ligament. And that way, it's surrounding the tendon as a synovial sheet of the intertubercular sulcus or groove. Now, it is time for us to talk about the blood supply of the shoulder joint. There are few vessels that we need to discuss. The first one is the anterior, this is on the anterior side and is highlighted in blue here. This small artery here is known as the anterior circumflex humeral artery, and it originates from the axillary artery right here. And the other one that is also supplying the shoulder joint is on the posterior side, and this is the posterior circumflex humeral artery highlighted in green. Now, the other one that is also a major blood supplier of the shoulder joint is this one here, this small vessel here, highlighted in yellow. This is the suprascapular artery and originates from the subclavian artery. The shoulder joint also has a nerve supply, and I wanted to briefly discuss here on this tutorial. What we have here is two views, the anterior... or posterior view (sorry) on your left and the anterior view here on your right. And the first nerve that we're going to discuss is the axillary nerve, and I have it here highlighted in green. As you can see, this is the structure that is passing through all or alongside these structures that I left so you can have an idea of the relation of the axillary nerve to the other structures on the shoulder joint. And on the anterior view, you can also see, highlighted in green, the axillary nerve that comes off the brachial plexus from the upper trunk posterior division and posterior cord, but I don't want to go into details. I will do a tutorial on the brachial plexus later on. But this is just to know that the axillary nerve also carries fibers from C5 and C6. The next structure, the next nerve that we will talk about—this is the second one and the last one that I want to cover on this tutorial—is the suprascapular nerve, and you have two posterior views so you can see the suprascapular nerve, also highlighted in green. You can see it also on your right and with more structures involved so you can see how it relates to them. And this suprascapular nerve arises from the upper trunk, and it's formed by the union of the fifth and the sixth cervical nerves or fibers. Now for the last part of this tutorial, I want to briefly discuss the movements associated to the shoulder joint. And as I mentioned before, this is one of the most mobile joints that you have in your body. As you're watching, now, this tutorial, I suggest you move your shoulder as much as you want or move your arm as much as you want. That's thanks to this very mobile joint. Now, the movements that we are just going to briefly touch are the abduction and adduction. As you're seeing the arrows, this is where to movement will occur. Now, the other two are flexion, which is forward lifting of the arm, and extension, which we would say is backward lifting of the arm. Now, you also have internal or medial rotation, and external or lateral rotation. You do have elevation which is excessive associated scapular movement, which will happen with abduction of more than 90 degrees—say if you're lifting your arm high enough to hail a cab or a taxi. And this happens because... We call it excessive, let's say, because the joint movement is restricted by the coracoacromial ligament that you have here. So it's restricted by this ligament right here. Now, the last movement that we're going to talk about is known as circumduction. And this is a combination of movements such as flexion, extension, and abduction, and adduction. Now that you'd just completed this video tutorial, then it's time for you to continue your learning experience by testing and also applying your knowledge. There are three ways you can do so here at Kenhub. The first one is by clicking on our "start training" button, the second one is by browsing through our related articles library, and the third one is by checking out our atlas. Now, good luck everyone, and I will see you next time. https://www.kenhub.com
Membranes
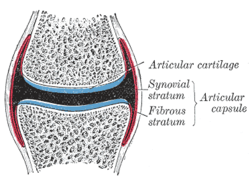
Each capsule consists of two layers or membranes:
- an outer (fibrous membrane, fibrous stratum) composed of avascular white fibrous tissue
- an inner (synovial membrane, synovial stratum) which is a secreting layer
On the inside of the capsule, articular cartilage covers the end surfaces of the bones that articulate within that joint.
The outer layer is highly innervated by the same nerves which perforate through the adjacent muscles associated with the joint.
Fibrous membrane
The fibrous membrane of the joint capsule is attached to the whole circumference of the articular end of each bone entering into the joint, and thus entirely surrounds the articulation. It is made up of dense connective tissue. It's a long spongy tissue.
Clinical significance
Frozen shoulder (adhesive capsulitis) is a disorder in which the shoulder capsule becomes inflamed.
Plica syndrome is a disorder in which the synovial plica becomes inflamed and causes abnormal biomechanics in the knee.
Gallery
-
 Left clavicle. Inferior surface.
Left clavicle. Inferior surface. -
 Right hip bone. External surface.
Right hip bone. External surface. -
 Right knee in extension. Deep dissection. Posterior view.
Right knee in extension. Deep dissection. Posterior view. -
 Right knee in extension. Deep dissection. Posterior view.
Right knee in extension. Deep dissection. Posterior view.

See also
- Articular capsule of the humerus
- Articular capsule of the knee joint
- Atlanto-axial joint
- Capsule of atlantooccipital articulation
- Capsule of hip joint
- Capsule of temporomandibular joint
References
![]() This article incorporates text in the public domain from page 282 of the 20th edition of Gray's Anatomy (1918)
This article incorporates text in the public domain from page 282 of the 20th edition of Gray's Anatomy (1918)
- ^ eMedicine/Stedman Medical Dictionary Lookup! Archived 2008-04-12 at the Wayback Machine
External links
- Cross section image: pelvis/pelvis-e12-15—Plastination Laboratory at the Medical University of Vienna
| National | |
|---|---|
| Other | |