
| XMEN disease | |
|---|---|
| Other names | Combined immunodeficiency due to MAGT1 deficiency |
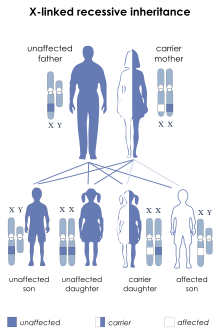 | |
| X-linked recessive is the manner in which this condition is inherited. | |
XMEN disease is a rare genetic disorder of the immune system that illustrates the role of glycosylation in the function of the immune system. XMEN stands for “X-linked MAGT1 deficiency with increased susceptibility to Epstein–Barr virus (EBV) infection and N-linked glycosylation defect.[1]” The disease is characterized by CD4 lymphopenia, severe chronic viral infections, and defective T-lymphocyte activation. Investigators in the laboratory of Dr. Michael Lenardo, National Institute of Allergy and Infectious Diseases at the National Institutes of Health first described this condition in 2011.[2][3][4]
YouTube Encyclopedic
-
1/3Views:4 3481 5981 040
-
Discovering XMEN Disease
-
Treating DOCK8 Deficiency at NIAID
-
Treating PASLI Disease
Transcription
Hunter and Parker Grove look like typical healthy little boys, but this could change at any time. The brothers are susceptible to recurring, severe infections with Epstein-Barr virus or EBV. Parents Lisa and Ian didn’t know why their sons kept having these infections. They only knew that their boys might each need a bone marrow transplant to address the condition. It’s a hard pill swallow to look at that kind of a treatment and why you’re doing it. And we would just pray “Please, if we could just hold on long enough to figure out what this is,” to have the confidence going into something that. And that’s what it’s given us. At the National Institute of Allergy and Infectious Diseases, federal government researchers study rare diseases that affect families like the Groves. Senior investigator Mike Lenardo and grad student Feng-Yen Li found that a mutated magnesium transport gene was causing the brothers’ condition. We examine families that have children that have deficits in the immune system or abnormalities of immune homeostasis – they have too many lymphocytes growing, sometimes that leads to cancer. And our job in analyzing those families is to try and understand the genetic basis of their disease because these are inherited disorders that the children are born with. As an outgrowth of that program, we came in contact with the Grove family. They had gone to several different medical centers in the U.S., and they’ve not gotten an explanation for why their children were sick; there were two boys in the family that were affected. And so we decided to use our knowledge and some new technologies to try and get to the basis of what was causing their disease. The study team named the boys’ condition XMEN disease, for X-linked magnesium deficiency with EBV and neoplasia. The good thing is both of them are still very young and very healthy of course, which continues to be the head scratcher, I guess, in this deal is why would you put them through so much when they look and act the way they do, so it’s kind of complicated. XMEN disease puts the boys at risk of cancer, so the Groves still need to decide about the transplant. But they’re relieved to finally have a diagnosis. You have to have a lot of patience. We’ve been coming here for almost 5 years. It’s just been a steady progress…patience and belief that you know that who you’re with and what you’re doing is the right thing. We know there’s nowhere else in the world that we’d rather be than here because of who we work with and what they’ve done for our family. It’s pretty special.
Presentation

XMEN patients have splenomegaly, chronic Epstein Barr Virus (EBV) infection, and are developmentally normal. They have an increased susceptibility for developing EBV+ lymphoma. Additionally, XMEN patients have excessive infections consistent with the underlying immunodeficiency. These infections included recurrent otitis media, sinusitis, viral pneumonia, diarrhea, upper respiratory infections, epiglottitis, and pertussis. Although autoimmune symptoms do not feature prominently in XMEN autoimmune cytopenias were observed in two unrelated patients.[2]
In the figure to the left, major features are present in all XMEN patients, while minor features are found only in some.
Genetics
XMEN disease is caused by loss of function mutations in the gene MAGT1.[2] MAGT1 is a 70 kb gene with 10 exons encoding for a 335 amino acid protein that maps to Xq21.1.[5] MagT1 is a component of the N-linked glycosylation machinery (oligosacchyrltransferase, OST), a fundamental component of all cells that regulates the attachment of sugar moieties onto specific sites in proteins. Many of the immunodeficiency-related features of XMEN disease are related to the hypoglycosylation phenotype caused by loss of the OST component MagT1.[6][7]
The conclusive connection between MAGT1, glycosylation, and Mg2+ import remains unknown. A prominent hypothesis from XMEN patients suggests that MAGT1's role in glycosylation is essential to the function (either directly or indirectly) of a Mg+2 transporter.[6][7]
MAGT1 is evolutionarily conserved and expressed in all mammalian cells with higher expression in hematopoietic lineages.[8] XMEN patients have been found to carry both MAGT1 deletions and missense mutations. However, the severity of the phenotype is not entirely explained by the genotype. The disease severity also likely depends on environmental and other genetic factors.[4]
XMEN disease follows an X-linked inheritance pattern because the MAGT1 is located on the X chromosome. Mothers of XMEN patients exhibit preferential X chromosome inactivation of the chromosome with the mutation in their hematopoietic cells and are asymptomatic.
Diagnosis
XMEN patients generally have chronically high levels of EBV with increased EBV-infected cells, diminished thymic output of CD4+ cells, reduced CD4:CD8 ratio, moderately high B cell counts, and mild neutropenia. Their neutropenia may be related to their chronic EBV. Some patients also showed defective T cell proliferation in response to mitogen stimulation, variable immunoglobulin deficiencies, or deficient vaccination response.[2][3][4]
Treatment
Once a diagnosis is made, each individual's treatment is based on an individual's clinical condition. Hematopoietic stem cell transplant is a possible treatment of this condition but its effectiveness is unproven and may be accompanied by severe and potentially fatal hemorrhage.[9][10]
It was previously thought magnesium supplementation was a promising potential treatment for XMEN.[4] One of the consequences of loss of MAGT1 function is a decreased level of unbound intracellular Mg2+. This decrease leads to loss of expression of an immune cell receptor called NKG2D, which is involved in EBV-immunity. Mg2+ supplementation in some tests restored NKG2D expression and other functions that are abnormal in patients with XMEN disease. Early evidence suggested continuous oral magnesium threonate supplementation was safe and well tolerated.[3] A randomized, double-blind, placebo-controlled, crossover study was conducted to evaluate the use of Mg2+ as a treatment for XMEN.[1] In vitro magnesium supplementation experiments failed to significantly rescue NKG2D expression in patients with XMEN disease and the clinical trial was stopped. Therefore, magnesium supplementation is unlikely to be an effective therapeutic option in XMEN disease.[1] Investigators at the National Institute of Allergy and Infectious Diseases at the US National Institutes of Health currently have clinical protocols to study new approaches to the diagnosis and treatment of this disorder.[11][12]
References
- ^ a b c Chauvin, Samuel D.; Price, Susan; Zou, Juan; Hunsberger, Sally; Brofferio, Alessandra; Matthews, Helen; Similuk, Morgan; Rosenzweig, Sergio D.; Su, Helen C.; Cohen, Jeffrey I.; Lenardo, Michael J. (2021-10-16). "A Double-Blind, Placebo-Controlled, Crossover Study of Magnesium Supplementation in Patients with XMEN Disease". Journal of Clinical Immunology. 42 (1): 108–118. doi:10.1007/s10875-021-01137-w. ISSN 1573-2592. PMC 10655616. PMID 34655400. S2CID 239004635.
- ^ a b c d Li FY, Chaigne-Delalande B, Kanellopoulou C, Davis JC, Matthews HF, Douek DC, et al. (July 2011). "Second messenger role for Mg2+ revealed by human T-cell immunodeficiency". Nature. 475 (7357): 471–6. doi:10.1038/nature10246. PMC 3159560. PMID 21796205.
- ^ a b c Chaigne-Delalande B, Li FY, O'Connor GM, Lukacs MJ, Jiang P, Zheng L, et al. (July 2013). "Mg2+ regulates cytotoxic functions of NK and CD8 T cells in chronic EBV infection through NKG2D". Science. 341 (6142): 186–91. Bibcode:2013Sci...341..186C. doi:10.1126/science.1240094. PMC 3894782. PMID 23846901.
- ^ a b c d e Li FY, Chaigne-Delalande B, Su H, Uzel G, Matthews H, Lenardo MJ (April 2014). "XMEN disease: a new primary immunodeficiency affecting Mg2+ regulation of immunity against Epstein-Barr virus". Blood. 123 (14): 2148–52. doi:10.1182/blood-2013-11-538686. PMC 3975255. PMID 24550228.
- ^ Goytain A, Quamme GA (April 2005). "Identification and characterization of a novel mammalian Mg2+ transporter with channel-like properties". BMC Genomics. 6 (48): 48. doi:10.1186/1471-2164-6-48. PMC 1129089. PMID 15804357.
- ^ a b Matsuda-Lennikov M, Biancalana M, Zou J, Ravell JC, Zheng L, Kanellopoulou C, et al. (September 2019). "N-linked glycosylation and expression of immune-response genes". The Journal of Biological Chemistry. 294 (37): 13638–13656. doi:10.1074/jbc.RA119.008903. PMC 6746436. PMID 31337704.
- ^ a b Ravell JC, Matsuda-Lennikov M, Chauvin SD, Zou J, Biancalana M, Deeb SJ, et al. (January 2020). "Defective glycosylation and multisystem abnormalities characterize the primary immunodeficiency XMEN disease". The Journal of Clinical Investigation. 130 (1): 507–522. doi:10.1172/JCI131116. PMC 6934229. PMID 31714901.
- ^ Zhou H, Clapham DE (September 2009). "Mammalian MagT1 and TUSC3 are required for cellular magnesium uptake and vertebrate embryonic development". Proceedings of the National Academy of Sciences of the United States of America. 106 (37): 15750–5. Bibcode:2009PNAS..10615750Z. doi:10.1073/pnas.0908332106. PMC 2732712. PMID 19717468.
- ^ Dimitrova, Dimana; Rose, Jeremy J.; Uzel, Gulbu; Cohen, Jeffrey I.; Rao, Koneti V.; Bleesing, Jacob H.; Kanakry, Christopher G.; Kanakry, Jennifer A. (January 2019). "Successful Bone Marrow Transplantation for XMEN: Hemorrhagic Risk Uncovered". Journal of Clinical Immunology. 39 (1): 1–3. doi:10.1007/s10875-018-0573-0. ISSN 1573-2592. PMID 30470981. S2CID 53717766.
- ^ Ravell, Juan C.; Chauvin, Samuel D.; He, Tingyan; Lenardo, Michael (2020-07-01). "An Update on XMEN Disease". Journal of Clinical Immunology. 40 (5): 671–681. doi:10.1007/s10875-020-00790-x. ISSN 1573-2592. PMC 7369250. PMID 32451662.
- ^ Clinical trial number NCT00001467 for "Genetic Analysis of Immune Disorders" at ClinicalTrials.gov
- ^ Clinical trial number NCT00246857 for "Screening Protocol for Genetic Diseases of Lymphocyte Homeostasis and Programmed Cell Death" at ClinicalTrials.gov