
Tetraplegia, also known as quadriplegia, is defined as the dysfunction or loss of motor and/or sensory function in the cervical area of the spinal cord.[1] A loss of motor function can present as either weakness or paralysis leading to partial or total loss of function in the arms, legs, trunk, and pelvis; paraplegia is similar but affects the thoracic, lumbar, and sacral segments of the spinal cord and arm function is retained.[1] The paralysis may be flaccid or spastic.[2] A loss of sensory function can present as an impairment or complete inability to sense light touch, pressure, heat, pinprick/pain, and proprioception.[1] In these types of spinal cord injury, it is common to have a loss of both sensation and motor control.
| Tetraplegia | |
|---|---|
| Other names | Quadriplegia |
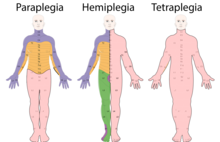 | |
| Affected areas (pink) representing differences between paraplegia (left), hemiplegia (middle), and tetraplegia (right). Areas may differ for each condition and are dependent upon level of injury. | |
| Specialty | Neurosurgery, Physical medicine & rehabilitation |
| Types | Complete, incomplete |
| Causes | Damage to spinal cord or brain by illness or injury; congenital conditions |
| Diagnostic method | Based on symptoms, medical imaging |
YouTube Encyclopedic
-
1/5Views:316 43227 58176 22314 752315
-
Aerobic Exercise for Individuals with Tetraplegia
-
spinal cord injury part-1/ classification/ paraplegia/ quadriplegia
-
Man with quadriplegia employs injury bridging technologies to move again - just by thinking
-
Paraplegia x Tetraplegia
-
Management of Tetraplegia
Transcription
Signs and symptoms
Although the most obvious symptom is impairment of the limbs, functioning is also impaired in the trunk and pelvic organs. This can lead to loss or impairment of controlling bowel and bladder, sexual function, digestion, breathing and other autonomic functions. Furthermore, sensation is usually impaired in affected areas. This may manifest as numbness, reduced sensation or neuropathic pain.[3] Secondarily, because of their depressed functioning and immobility, tetraplegics are often more vulnerable to pressure sores, osteoporosis and fractures, frozen joints, spasticity, respiratory complications, infections, autonomic dysreflexia, deep vein thrombosis, and cardiovascular disease.[4]
The severity of the condition depends on both the level at which the spinal cord is injured and the extent of the injury. An individual with an injury at C1 (the highest cervical vertebra, at the base of the skull) will probably lose function from the neck down and be ventilator-dependent. An individual with a C7 injury may lose function from the chest down but still retain use of the arms and much of the hands. An individual in between, with a C5 injury may lose some function from the chest down and fine motor skills in his/her hands but still have flexion and extension abilities of certain muscles around the back or arm area.
The extent of the injury is also important. A complete severing of the spinal cord will result in complete loss of function from that vertebra down. A partial severing or even bruising of the spinal cord results in varying degrees of mixed function and paralysis. A common misconception with tetraplegia is that the victim cannot move legs, arms, or any other major body regions; this is often not the case. Some tetraplegics can walk and use their hands, as though they did not have a spinal cord injury, while others may use wheelchairs and retain some functions in their arms and fingers; again, this varies based on the degree of damage to the spinal cord and is mostly seen with incomplete tetraplegia.[3]
It is common to have partial movement in limbs, such as the ability to move the arms but not the hands, or to be able to use the fingers but not to the same extent as before the injury. Furthermore, the deficit in the limbs may not be the same on both sides of the body; either side may be more affected, depending on the location of the lesion on the spinal cord.[3]
Another important factor is the possibility that the patient may exhibit sporadic movement in the affected areas. One of the main causes for this would be myoclonus, or muscle spasms. "After a spinal cord injury, the normal flow of signals is disrupted, and the message does not reach the brain. Instead, the signals are sent back to the motor cells in the spinal cord and cause a reflex muscle spasm. This can result in a twitch, jerk or stiffening of the muscle."[5]
Causes
Tetraplegia is caused by damage to the brain or the spinal cord at a high level. The injury, which is known as a lesion, causes the loss of partial or total function of all four limbs, meaning the arms and the legs. Typical causes of this damage are trauma (such as a traffic collision, diving into shallow water, a fall, a sports injury), disease (such as transverse myelitis, Guillain–Barré syndrome, multiple sclerosis, or polio), or congenital disorders (such as muscular dystrophy).[6]
| Cause | Conditions |
|---|---|
| Trauma | Motor vehicle accident, falls, violence, recreational activity[6] |
| Congenital | Spina bifida, spinal muscular atrophy, cerebral palsy[6] |
| Vascular | Ischemia due to arterial (aortic dissection, atherosclerosis, embolus), venous (thrombosis), or combined (AV malformation) causes[6] |
| Degenerative | Amyotrophic lateral sclerosis[6] |
| Infectious | Transverse myelitis (from viral, bacterial, or fungal source)[6] |
| Demyelinating | Multiple sclerosis, Guillain–Barré syndrome[6] |
Tetraplegia is defined in many ways; C1–C4 usually affects arm movement more so than a C5–C7 injury; however, all tetraplegics have or have had some kind of finger dysfunction. So, it is not uncommon to have a tetraplegic with fully functional arms but no nervous control of their fingers and thumbs. It is possible to have a broken neck without becoming tetraplegic if the vertebrae are fractured or dislocated but the spinal cord is not damaged. Conversely, it is possible to injure the spinal cord without breaking the spine, for example when a ruptured disc or bone spur on the vertebra protrudes into the spinal column.
Anatomy and function
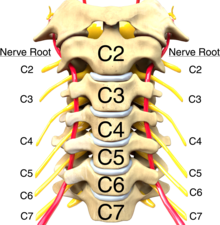
Since tetraplegia is defined as dysfunction in the cervical spinal cord, this section will focus on the anatomy of the cervical spinal cord. To understand how tetraplegia presents after injury, it is imperative to have a broad knowledge of the cervical spinal roots and its many functions. In the cervical spine, nerve roots exit the spine above the associated vertebra (i.e. the C6 nerve root exits above the C6 vertebra). By evaluating what nerve root of the cervical spine is injured, the affected muscle groups and dermatomes can be determined. This informs the evaluator as to what activities may be limited as a result of the injury. This is typically done at 72 hours post-injury; exams done prior to this time have been found to be inaccurate due to the presence of swelling and other confounding factors.[7] For example, an injury at the C6 nerve root level will affect the function of the triceps (elbow extension) but the biceps (elbow flexion) will be spared; in this case, an injury at the C6 root level affects all function at that level and below whereas the C5 nerve root, which controls the biceps, is spared since it is above the C6 level in the spinal column. When classifying an individual's level of function, there are numerous functional assessment tools that may be used in a clinical setting and it is often up to the clinician's discretion as to which tools are used. A comprehensive list of these tools may be found on the ShirleyRyan AbilityLab website.
| Root | Muscle Group | Root | Sensory Point |
|---|---|---|---|
| C2 | - | C2 | > 1 cm lateral to the occipital condyle |
| C3 | - | C3 | supraclavicular fossa at the midclavicular line |
| C4 | - | C4 | Over the acromioclavicular joint |
| C5 | Elbow flexors | C5 | Lateral antecubital fossa |
| C6 | Wrist extensors | C6 | Dorsal thumb |
| C7 | Elbow extensors | C7 | Dorsal middle finger |
| C8 | Long finger flexors | C8 | Dorsal little finger |
| T1 | Small finger abductors | T1 | Medial epicondyle of the elbow |
| T2 | - | T2 | Apex of the axilla |
Diagnosis
Classification
Spinal cord injuries are classified as complete and incomplete by the American Spinal Injury Association (ASIA) classification.[1] The ASIA scale grades patients based on their functional impairment as a result of the injury, grading a patient from A to D. This has considerable consequences for surgical planning and therapy.[8] After a comprehensive neurologic exam testing segments of the body corresponding to spinal nerve roots, the examiner will determine the patient's motor level and sensory level (i.e. motor level C6, sensory level C7). These levels are unique for the patient's left and right side. This level is assigned based on the lowest (closest to the patient's feet) intact motor and sensory level. After this assignment, a neurological level of injury (NLI) is determined. The NLI is the lowest segment with intact sensory and motor function provided there is normal sensory and motor function above this segment.[1]
| American Spinal Injury Association Impairment Scale[8] | ||
|---|---|---|
| A | Complete | No motor or sensory function is preserved in the sacral segments S4–S5. |
| B | Incomplete | Sensory but not motor function is preserved at S4–S5. No motor function is preserved >3 levels below the motor neurological level of injury. |
| C | Incomplete | Motor function is preserved below the neurological level; more than half of key muscles below the neurological level have a muscle grade less than 3. |
| D | Incomplete | Motor function is preserved below the neurological level; at least half of key muscles below the neurological level have a muscle grade of 3 or more. |
Complete spinal-cord lesions
As in the above ASIA chart, a complete spinal cord injury is any injury which has absent motor and sensory function in the sacral segments S4 and S5. This is verified during the physical exam by the absence of all three of: voluntary anal contraction, deep anal pressure, and pinprick+light touch sensation in the perineal area.[1] S4 and S5 are both sacral nerve roots found at the lowest portion of the spinal cord. In simpler terms, "complete" is meant as a way to express that the spinal cord is injured such that no signal, motor or sensory, is carried to or from the level of injury to these lower levels of the spinal cord.
Incomplete spinal-cord lesions
Incomplete spinal cord injuries result in varied post injury presentations. There are three main syndromes described, depending on the exact site and extent of the lesion.
- Central cord syndrome: an injury to the central area of the spinal cord, most often seen as a result of a fall with subsequent hyperextension injury. This typically presents with weakness greater in the upper limbs than in the lower limbs.[1]
- Brown-Séquard syndrome: hemisection of the spinal cord with resultant loss in: a.) ipsilateral proprioception, vibration, and motor control below the level of injury b.) complete sensory loss at the level of injury c.) contralateral pain and temperature loss.[1]
- Anterior cord syndrome: a lesion of the anterior two-thirds of the spinal cord, most commonly due to ischemia. This typically presents with loss of pain, temperature, and motor function at and below the level of injury.[1]
- Cauda equina syndrome: a lesion of the lumbosacral nerve roots that may spare the spinal cord. As these nerve roots are lower motor neurons, a flaccid lower limb paralysis is typically seen along with loss of bowel and bladder reflexes, varying degrees of impairment of sensation, and loss of sacral reflexes (bulbocavernosus reflex, anal wink).[1]
- Conus medullaris syndrome: a lesion similar to cauda equina syndrome however this lesion is typically found higher in the cord. This presents clinically similarly to cauda equina syndrome however there may be intact sacral reflexes. Unlike cauda equina, the unique location of this syndrome leads it to present with mixed upper and lower motor neuron signs.[1]
For most patients with ASIA A (complete) tetraplegia, ASIA B (incomplete) tetraplegia and ASIA C (incomplete) tetraplegia, the International Classification level of the patient can be established without great difficulty. The surgical procedures according to the International Classification level can be performed. In contrast, for patients with ASIA D (incomplete) tetraplegia it is difficult to assign an International Classification other than International Classification level X (others).[9] Therefore, it is more difficult to decide which surgical procedures should be performed. A far more personalized approach is needed for these patients. Decisions must be based more on experience than on texts or journals.[9]
The results of tendon transfers for patients with complete injuries are predictable. On the other hand, it is well known that muscles lacking normal excitation perform unreliably after surgical tendon transfers. Despite the unpredictable aspect in incomplete lesions, tendon transfers may be useful. The surgeon should be confident that the muscle to be transferred has enough power and is under good voluntary control. Pre-operative assessment is more difficult to assess in incomplete lesions.[9]
Patients with an incomplete lesion also often need therapy or surgery before the procedure to restore function to correct the consequences of the injury. These consequences are hypertonicity/spasticity, contractures, painful hyperesthesias and paralyzed proximal upper limb muscles with distal muscle sparing.[9]
Spasticity is a frequent consequence of incomplete injuries. Spasticity often decreases function, but sometimes a patient can control the spasticity in a way that it is useful to their function. The location and the effect of the spasticity should be analyzed carefully before treatment is planned. An injection of botulinum toxin (Botox) into spastic muscles is a treatment to reduce spasticity. This can be used to prevent muscle shortening and early contractures.[2][9]
Over the last ten years, an increase in traumatic incomplete lesions is seen, due to the better protection in traffic.
Treatment
Upper limb paralysis refers to the loss of function of the elbow and hand. When upper limb function is absent as a result of a spinal cord injury it is a major barrier to regain autonomy. People with tetraplegia should be examined and informed concerning the options for reconstructive surgery of the tetraplegic arms and hands.[10]
Prognosis

Delayed diagnosis of cervical spine injury has grave consequences for the victim. About one in 20 cervical fractures are missed and about two-thirds of these patients have further spinal-cord damage as a result. About 30% of cases of delayed diagnosis of cervical spine injury develop permanent neurological deficits. In high-level cervical injuries, total paralysis from the neck can result. High-level tetraplegics (C4 and higher) will likely need constant care and assistance in activities of daily living (ADLs), such as getting dressed, eating, and bowel/bladder care. Individuals with C5 injuries retain some function in their biceps, deltoids, and other muscles; they typically can perform many ADLs including feeding, bathing, and grooming but require total assistance with bowel/bladder care. The C6 level adds function in the extensor carpi radialis, longus, and other muscles allowing for wrist extension, scapular abduction, and wrist flexion; typically, these patients have modified independent feeding and grooming with adaptive equipment, independent with dressing, can use both a manual and power wheelchair but require assistance with some activities of daily living. The C7 level is where function is retained in the triceps allowing for arm extension; C7 is considered the key level at which most activities can be performed independently with a wheelchair and assistive devices; activities include feeding, grooming, dressing, light meal preparation, and transfers on level surfaces.[3] Even in complete spinal cord injury, it is common for individuals to recover up to 1 level of motor function.[7]
Even with "complete" injuries, in some rare cases, through intensive rehabilitation, function can be regained through "rewiring" neural connections, as in the case of actor Christopher Reeve.[11]
In the case of cerebral palsy, which is caused by damage to the motor cortex either before, during (10%), or after birth, some people with incomplete tetraplegia are gradually able to learn to stand or walk through physical therapy.[3]
Tetraplegics can improve muscle strength by performing resistance training at least three times per week. Combining resistance training with proper nutrition intake can greatly reduce co-morbidities such as obesity and type 2 diabetes.[12]
Epidemiology
There are an estimated 17,700 spinal cord injuries each year in the United States; the total number of people affected by spinal cord injuries is estimated to be approximately 290,000 people.[13]
In the US, spinal cord injuries alone cost approximately $40.5 billion each year, which is a 317 percent increase from costs estimated in 1998 ($9.7 billion).[14]
The estimated lifetime costs for a 25-year-old in 2018 is $3.6 million when affected by low tetraplegia and $4.9 million when affected by high tetraplegia.[13] In 2009, it was estimated that the lifetime care of a 25-year-old rendered with low tetraplegia was about $1.7 million, and $3.1 million with high tetraplegia.[15]
About 1,000 people are affected each year in the UK (~1 in 60,000—assuming a population of 60 million).
Terminology
The condition of paralysis affecting four limbs is alternately termed tetraplegia or quadriplegia. Quadriplegia combines the Latin root quadra, for "four", with the Greek root πληγία plegia, for "paralysis". Tetraplegia uses the Greek root τετρα tetra for "four". In the past, "tetraplegia" and "quadriplegia" were used interchangeably in the medical literature. Medical literature favors using "tetraplegia" as the standardized term, as it is frowned upon to mix Greek and Latin roots, although "quadriplegia" remains in use.[16]
"Tetraplegia", meaning the paralysis of four limbs, may be confused with "tetraparesis", meaning the weakness of four limbs. In medicine, it is important to not use these terms when making a diagnosis. When diagnosing and classifying spinal cord injuries, the ASIA classification is used to distinguish between weakness vs. no weakness, and to classify neurologically complete vs. incomplete lesions. Use of "tetraparesis" is discouraged as it inaccurately describes an incomplete lesion and incorrectly implies tetraplegia applies only to cases of complete lesions.[17]
See also
- Clearing the cervical spine
- Hemiplegia
- Paraplegia
- Locked-in syndrome
- Sexuality after spinal cord injury
- Spinal cord injury research
References
- ^ a b c d e f g h i j k Rupp R, Biering-Sørensen F, Burns SP, Graves DE, Guest J, Jones L, et al. (2021-03-01). "International Standards for Neurological Classification of Spinal Cord Injury: Revised 2019". Topics in Spinal Cord Injury Rehabilitation. 27 (2): 1–22. doi:10.46292/sci2702-1. PMC 8152171. PMID 34108832.
- ^ a b Adams MM, Hicks AL (October 2005). "Spasticity after spinal cord injury". Spinal Cord. 43 (10): 577–586. doi:10.1038/sj.sc.3101757. PMID 15838527. S2CID 2659838.
- ^ a b c d e f Spinal cord medicine. Steven Kirshblum, Vernon W. Lin (3rd ed.). New York. 2019. ISBN 978-0-8261-3775-3. OCLC 1079055185.
{{cite book}}: CS1 maint: location missing publisher (link) CS1 maint: others (link) - ^ Schurch B, Knapp PA, Jeanmonod D, Rodic B, Rossier AB (January 1998). "Does sacral posterior rhizotomy suppress autonomic hyper-reflexia in patients with spinal cord injury?". British Journal of Urology. 81 (1): 73–82. doi:10.1046/j.1464-410x.1998.00482.x. PMID 9467480.
- ^ "Spasticity and Spinal Cord Injury | Model Systems Knowledge Translation Center (MSKTC)". msktc.org. Retrieved 2022-10-03.
- ^ a b c d e f g McDonald JW, Sadowsky C (February 2002). "Spinal-cord injury". Lancet. 359 (9304): 417–425. doi:10.1016/S0140-6736(02)07603-1. PMID 11844532.
- ^ a b Chay, Wesley; Kirshblum, Steven (2020-08-01). "Predicting Outcomes After Spinal Cord Injury". Physical Medicine and Rehabilitation Clinics of North America. 31 (3): 331–343. doi:10.1016/j.pmr.2020.03.003. ISSN 1047-9651. PMID 32624098. S2CID 219735858.
- ^ a b Roberts TT, Leonard GR, Cepela DJ (May 2017). "Classifications In Brief: American Spinal Injury Association (ASIA) Impairment Scale". Clinical Orthopaedics and Related Research. 475 (5): 1499–1504. doi:10.1007/s11999-016-5133-4. PMC 5384910. PMID 27815685.
- ^ a b c d e Hentz VR, Leclercq C (May 2008). "The management of the upper limb in incomplete lesions of the cervical spinal cord". Hand Clinics. 24 (2): 175–84, vi. doi:10.1016/j.hcl.2008.01.003. PMID 18456124.
- ^ Fridén J, Reinholdt C (2008). "Current concepts in reconstruction of hand function in tetraplegia". Scandinavian Journal of Surgery. 97 (4): 341–6. doi:10.1177/145749690809700411. PMID 19211389.
- ^ Burkeman O (2002). "Man of steel". The Guardian. Retrieved 4 September 2018.
- ^ Gorgey AS, Mather KJ, Cupp HR, Gater DR (January 2012). "Effects of resistance training on adiposity and metabolism after spinal cord injury". Medicine and Science in Sports and Exercise. 44 (1): 165–74. doi:10.1249/MSS.0b013e31822672aa. PMID 21659900.
- ^ a b "National Spinal Cord Injury Statistical Center, Facts and Figures at a Glance" (PDF). Birmingham, AL: University of Alabama at Birmingham. 2018.
- ^ "Stats about paralysis". Christopher & Dana Reeve Foundation. 2016. Retrieved 4 September 2018.
- ^ "National Spinal Cord Injury Statistical Center, Facts and Figures at a Glance" (PDF). Birmingham, AL: University of Alabama at Birmingham. 2009.
- ^ Solinsky R, Kirshblum SC (November 2018). "Challenging questions regarding the international standards". The Journal of Spinal Cord Medicine. 41 (6): 684–690. doi:10.1080/10790268.2017.1362929. PMC 6217465. PMID 28820352.
- ^ Nas K, Yazmalar L, Şah V, Aydın A, Öneş K (January 2015). "Rehabilitation of spinal cord injuries". World Journal of Orthopedics. 6 (1): 8–16. doi:10.5312/wjo.v6.i1.8. PMC 4303793. PMID 25621206.
Further reading
- Taylor-Schroeder S, LaBarbera J, McDowell S, Zanca JM, Natale A, Mumma S, et al. (2011). "The SCIRehab project: treatment time spent in SCI rehabilitation. Physical therapy treatment time during inpatient spinal cord injury rehabilitation". The Journal of Spinal Cord Medicine. 34 (2): 149–61. doi:10.1179/107902611X12971826988057. PMC 3066500. PMID 21675354.
- "Quadriplegia and Tetraplegia". Apparelyzed – Spinal Cord Injury Peer Support. n.d. Archived from the original on 5 Jan 2014. Retrieved 4 September 2018.
{{cite web}}: CS1 maint: unfit URL (link)
External links
| National | |
|---|---|
| Other | |